Welcome to Bw Reads, our weekend newsletter featuring one great magazine story from Bloomberg Businessweek. Today Jason Gale and Jessica Nix write about how an Ebola strain with no known treatment or vaccine is spreading fast, and why the international system built to contain outbreaks is in crisis. You can find the whole story online (free) here or you can listen to it here. If you like what you see, tell your friends! Sign up here. As the burial workers in masks, gloves and blue surgical gowns pull a coffin from the back of a vehicle, the mourners press in closer. Yelling and gesturing, the crowd buffets and shoves the men. “Open it so we can see him! Open it so we can see him!” they shout. “You’re thieves!” onlookers cry. “You’ve killed someone!” With the pressure escalating, the team sets the coffin on the ground and steps back, allowing the lid to be opened. An Ebola patient’s viral load often peaks around the time of death, when infectious bodily fluids can almost coat the body, making touching a corpse especially dangerous. So these chaotic moments, captured in a shaky cellphone video from the town of Kyondo in the eastern Democratic Republic of Congo, risk becoming yet another axis of transmission in the growing outbreak. 
The confrontation isn’t an isolated event: Treatment tents and isolation wards have been set on fire, and tensions at one burial became so volatile that police fired warning shots into the air to disperse the crowd. In early June it was reported that a team conducting another burial had been attacked, forcing workers to abandon the coffin. This violence, stemming from mistrust of authorities, is hampering efforts to contain a particularly dire outbreak of Ebola, whose pathology — it can overwhelm the body with fever, vomiting, diarrhea, internal bleeding and organ failure — has made it one of the world’s most feared diseases. As of June 2, more than 470 suspected or confirmed cases and at least 61 deaths had been reported across a swath of Congo and Uganda stretching about as far as the distance from New York to Cleveland. 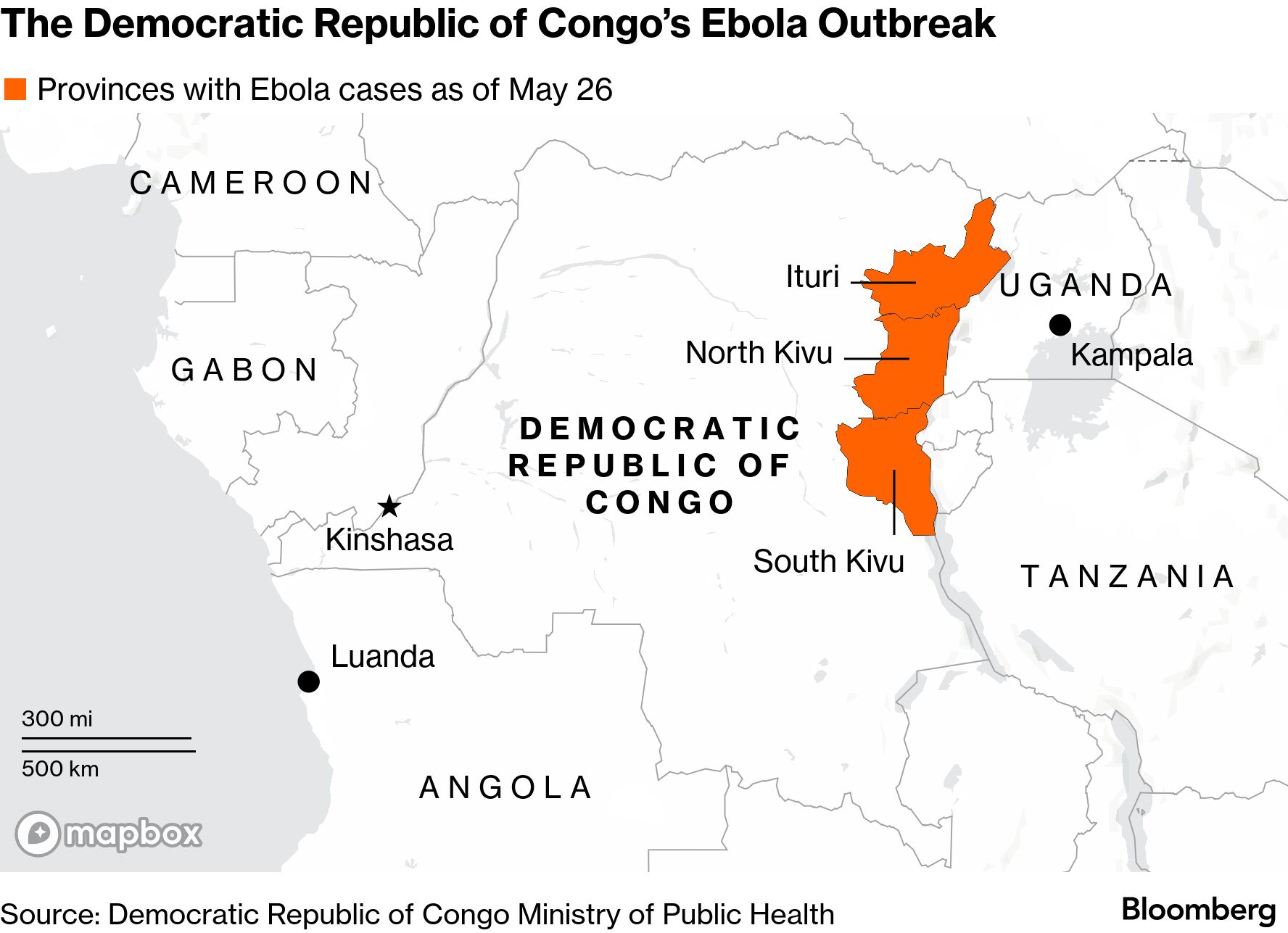
“This outbreak has the most momentum upon discovery of any Ebola outbreak in history,” says Jeremy Konyndyk, a former senior official with the US Agency for International Development who oversaw the American response to the 2014-16 West African Ebola epidemic. “It’s going to be exceptionally difficult to contain.” The world spent a decade overhauling Ebola preparedness after the West African epidemic, which was by far the deadliest on record. Even with a steady commitment to those reforms, though, the current outbreak would have been hard to stop. Much of the world’s planning focused on the more common Zaire strain, leading to vaccines, antibody treatments and rapid tests that have successfully disrupted several outbreaks. But the rarer Bundibugyo strain behind the current epidemic has no approved vaccine or treatment, and widely used diagnostic tools initially failed to detect it. The virus also surfaced in one of the hardest places in the world to stop an outbreak: a war-scarred region where years of conflict have displaced more than 5 million people, hollowed out health systems and frayed trust between communities and the government. 
Former USAID official Konyndyk.
Photographer: Jared Soares for Bloomberg Businessweek
Former US officials say the challenges were exacerbated by a foreign aid freeze announced by the Trump administration and the decimation of American-backed health programs under Elon Musk’s Department of Government Efficiency, which included the dismantling of USAID and the cancellation of almost 85% of its programs. Prior to that, in eastern Congo the agency funded health groups, community surveillance, specimen transport and monitoring of potential disease transmission from animals to humans. Other G7 countries also cut aid last year, including Germany, France, Japan and the UK, but none did so nearly as steeply as the US, whose annual global development assistance dropped by 57%, according to figures from the Organization for Economic Cooperation and Development. One flagship US program that supported related capacity across Africa, the $245 million Strides Initiative, was repeatedly halted and restarted, throwing contracts and payment systems into turmoil and prompting a major partner to lay off staff, according to a former senior USAID official who oversaw outbreak preparedness before leaving last year. US assistance to Congo has also fallen sharply since last year, including steep reductions in humanitarian and health programs tied to outbreak preparedness and response. Konyndyk says USAID’s former footprint in Congo gave American officials a much clearer picture of what was happening on the ground, especially in the conflict-hit east, where humanitarian funding was concentrated. Much of that “eyes and ears” capability disappeared after missions were closed and staff and funding were cut. “When I was at USAID, if my team had come to me and said, ‘Some of our NGO partners are seeing clusters of unexplained viral hemorrhagic fever in eastern Congo,’ that would be a hair-on-fire type of moment,” Konyndyk says. “Now many of those programs are gone, and there’s no one on the other end of the line in the US government.” Internal tensions over the cuts spilled into public view early on. In congressional testimony last March, Nicholas Enrich, USAID’s former acting assistant administrator for global health, said that after an Ebola outbreak was reported in Uganda in late January 2025, bureaucratic bottlenecks tied to the Trump administration’s foreign aid freeze slowed the response. (The outbreak was declared over that April.) Enrich also testified that political appointees had instructed staff to give lower priority to Ebola response work even after some programs resumed. The State Department disputed his account, telling Wired magazine that Secretary of State Marco Rubio personally reviewed and approved USAID decisions and that Enrich was spreading “leaks and lies.” Other parts of the global disease-response system were scaled back after the US began withdrawing from the World Health Organization in early 2025. Those cuts included a $35 million award supporting WHO emergency surveillance, laboratory networks and outbreak coordination. Funding was also cut for a WHO-managed global network of more than 700 laboratories that track pathogens including Ebola, dengue and measles. The organization has struggled to deal with the collapse of support from what had long been its largest donor. With other governments not stepping in to fully replace the lost funding, the WHO has frozen hiring, laid off staff and sharply reduced spending across emergency operations. Former US officials and on-the-ground partners say the result of these and other cuts has been a thinner, slower and more fragmented international response system, just as another major Ebola crisis unfolds.  
Video: The High Price of ‘America First’ Aid Deals
The Trump administration disputes claims that its policies have weakened outbreak detection, and Department of State officials have stressed that an epidemic emerging in a remote conflict zone would have been difficult to identify under any circumstances. White House spokesman Kush Desai said in a statement that within 24 hours of being notified of the outbreak, the administration “mobilized a swift and robust response: convening top medical experts, deploying aid and materiel, increasing screening and testing procedures, airlifting American citizens out of the DRC” and implementing travel restrictions. Desai added that the US “continues to act faster and more comprehensively than any other country to contain the transmission of Ebola.” Tommy Pigott, a spokesman for the State Department, says, “It is false to claim that the USAID reform has negatively impacted our ability to respond to Ebola.” The State Department added in a statement that the realignment of USAID “did not have any significant effect” on funding levels for health and health security programs in the eastern part of Congo, and that the US has recently mobilized more than $110 million in assistance to the country, where it “continues to be the largest bilateral donor.” The department added that Strides and similar programs are now overseen by its Bureau of Global Health Security and Diplomacy, a structure that provides “more efficient and effective coordination.” An internal WHO briefing note circulated in mid-May and viewed by Bloomberg Businessweek warned that aid cuts and conflict were pushing parts of eastern Congo’s health system toward collapse. More than half of health facilities in some areas had closed or been damaged, the note said, and as many as 85% of those that remained were facing critical drug and staff shortages, with almost 40% of health workers estimated to have left their posts. “We’re playing catch-up,” says Ciarán Donnelly, senior vice president for crisis response, recovery and development at the International Rescue Committee, which operates health sites in Congo. “Every delay in tackling any contagious outbreak — and especially Ebola — can be fatal.” The IRC, whose budget relies broadly on the US and other donors, has scaled back 60% of its Congolese health sites; in Bunia, the outbreak’s epicenter, only two of its five primary care sites remain. In the 10 days after the outbreak was declared, pharmacies in Bunia ran out of hand sanitizer, and local health officials reported shortages of protective equipment. The city’s laboratory was processing only a trickle of Ebola tests and briefly suspended operations after running out of fuel for a generator, aid workers told the New York Times. As for burials, Red Cross teams have people trained to carry out them out in a safe and dignified manner but lack the money to pay for the work, says Joanne Liu, a public-health professor at McGill University who helped lead Médecins Sans Frontières’ response to the West African epidemic. The result of all this is a dangerous convergence of crises: Ebola spreading through one of the hardest places in the world to contain it, at a moment when the international surveillance and response systems built after past epidemics are significantly weakened. “I suspect the numbers we have are only a fraction of the actual toll, and the limited testing and contact tracing suggest it will be early to mid-June before we have a realistic understanding of what’s happening on the ground,” says Craig Spencer, an emergency-medicine physician who became New York City’s first Ebola patient after treating cases in West Africa in 2014. “What we’re seeing now is really the worst-case scenario.”
Keep reading
On the PodcastIs YouTube the new film incubator? After two hit movies from internet-native directors, Bloomberg News’ Screentime writer Lucas Shaw joins the Everybody’s Business podcast to figure out if the buzz around Backrooms and Obsession is just a fluke or marks a trend. We also check in on the Iran conflict with Bloomberg Opinion columnist Javier Blas, and discuss why the expected global economic meltdown hasn’t materialized. Plus: Some clumsy alleged insider trading, and a couple of instances of international art theft. Listen and subscribe on Apple, Spotify, iHeart and the Bloomberg Terminal. More Weekend Reads

Watch The Deal: FIFA’s Jill Ellis on World Cup Demand
Play Alphadots!Our daily word puzzle with a plot twist. 
Today’s clue: Olympic torch bearer? More From BloombergLike Businessweek Daily? Check out these newsletters:
Explore all Bloomberg newsletters. We’re improving your newsletter experience and we’d love your feedback. If something looks off, help us fine-tune your experience by reporting it here. Follow Us You received this message because you are subscribed to Bloomberg’s Businessweek Daily newsletter. If a friend forwarded you this message, sign up here to get it in your inbox.
|
Sunday, June 7, 2026
Bw Reads: A world vulnerable to Ebola
Subscribe to:
Post Comments (Atom)
-
Bloomberg Evening Briefing Americas View in browser Who's paying for Donald Trum...
-
PLUS: Dogecoin scores first official ETP ...



No comments:
Post a Comment